9 - THE REMODELING OF THE BONE
Integration or osseointegration, if you prefer, is not forever but the body calls it into question every day. Very clear and exhaustive Misch describes something that is not a static picture but a real film. 235 paragraph: bone-implant interface notes: - the human cortical bone of the shaft of long bones and of the rib remodels with a percentage ranging from 2% to 10% per year .......... - The cortical bone that supports the teeth can essentially have a faster remodeling speed; (30-40% per year). - As shown in figure 17.9, the cortical bone around an endosseous implant continues to remodel. The long-term maintenance of rigid bone fixation involves a remodeling rate of about 500% per year of the immediately adjacent bone within 1mm of the implant. (from Roberts WE London 1993 Quintessence - Osseointegration in oral rehabilitation). Chiapasco reports similar percentages and the same values have been repeated in universities. Other than osseointegrated!
The most recent research indicates that there is an unstable balance that our bone guarantees us over time at the price of a fast and incessant replacement of the implant-bearing structures. These regrowth rates are disturbing, thinking of pathological tissues in which this characteristic is expressed to the maximum degree such as neoplasms. We must therefore be grateful to our dear normal bone for being able to cope with the chewing loads using structures foreign to it, only compatible metals, without the equipment supplied to us by mother nature: the periodontium, the splendid antibacterial shield that allows the painless discharge of the forces to he transmitted. The biological seal. On p. 249 Misch, speaking of the biological seal and in particular of the deformation to which the hemidesmosomes are subjected, says ..... 'it can be argued that a large diameter implant abutment will be more likely to suffer violations of this seal due to tissue stretching than a smaller diameter abutment. Clinically, stretching of the tissue around small diameter abutments is rarely observed, no matter if on cylindrical or blade implants, and in most subperiosteal implants, while it is a fairly common finding around larger diameter abutments. ' These considerations, repeated in other parts of the book, highlight that Misch knows the advantage of using small diameter implant necks as an alternative to large diameter ones in counteracting mucositis, peri-implant resorption and bone infections. Nonetheless, he opted for the second type of implant, attributing the crestal damage more to bacterial factors and occlusal stress. In our opinion, he did not sufficiently consider the pejorative contribution due to the design of the implant itself in its overall volume, in the length of its neck, in the size and pitch of its coils, in its internal spaces, in its surface roughness.
|
Date 11 \ 12 \ 2019 |
Carpenedolo Clinic |
|
surname and name: xxx |
Age 55 |
|
No. of existing plants 1 |
Date and number of interventions already made: October 2015 in 25 |
|
Type of plant: Tramonte |
N ° implants inserted: 3 |
|
Welding no |
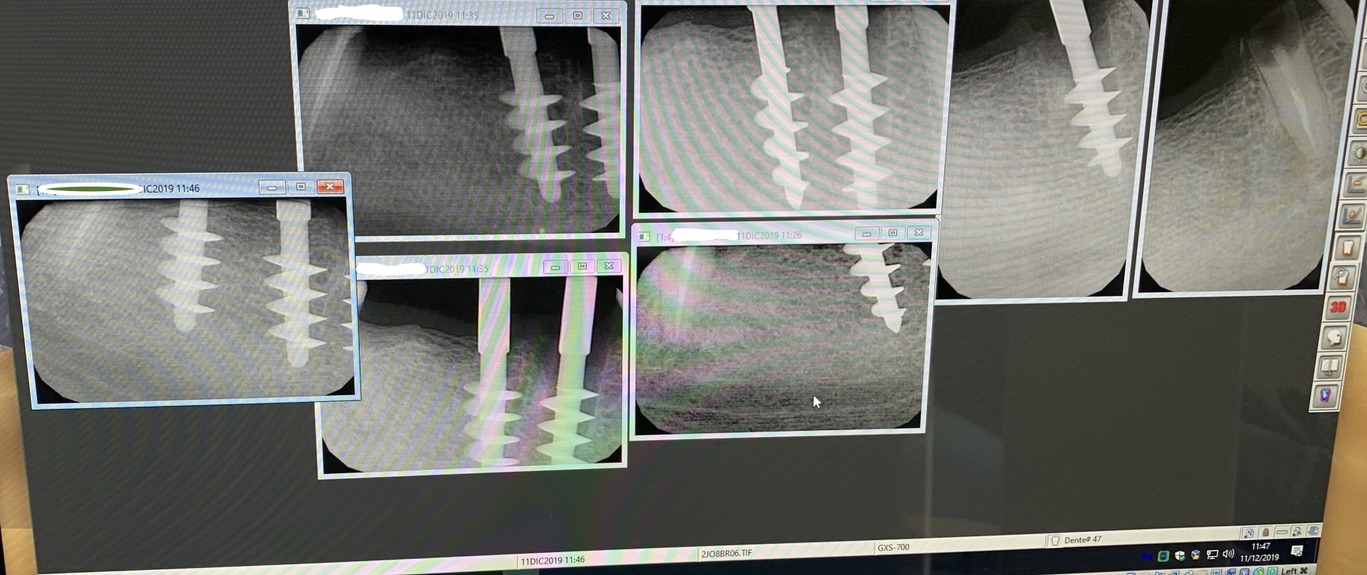
Dental area: 45 46 47 |
|
App. Intraoral Rx CDR Carpenedolo |
TAC: Yes Acquafredda |
|
Pexist mining situation in 45 and nopex in 46 and 47 |
Density according to Misch: 2 |
|
Natural elements antagonist, impl / mobile prosthesis: bridge on teeth and implants. |
Thick mucosa thickness medium thin: medium |
|
Chewing height high medium low Low |
Bruxism with window frames |
|
Photo: Iphone Xs |
Models: yes
|











STUDI DENTISTICI BAZZOLI e BELLINI
Privacy Policy e Cookie Policy
Internet Partner Global Informatica
![]()