5 - LONGEVITY OF THE IMPLANTS
News n. 5. 19/12/2020
Immediate post-extraction implants with immediate loading.
In many researches, articles and texts, referring to the years of the second half of the 1900s, we often speak of the dawn of implantology, almost as if they were a primitive period, now outdated, in the face of the admirable and progressive fate of implantology science, which has continuously progressed year after year since then.
But for those who lived and worked in those years, even if only partially like us, (I remember Prof. Ugo Pasqualini's first enrollment in SOMECOI in 1984), the awareness that the foundations of implant therapy have remained the same is still very lively.
Many fashions have proved to be fleeting, I am referring for example to surgical bone grafting techniques in the posterior sectors of the mouth. Instead, one of the fundamental principles of implantology, especially in Italy, was re-evaluated.
Recent research has shown that immediate and progressive loading constitutes a formidable contribution to the success and integration of the implant into the host bone.
Despite 30 years of prevailing Branemarkian philosophy, it is a satisfaction to remember that in the 2000s the essential value of immediate implant loading was recognized by the contemporary scientific community.
However, it is surprising that they want to do it using an inadequate technique to achieve this result.
Although official implantology has denied the categorical imperative of the Swedish and American school not to load the implant immediately but to leave it submerged and inactive for several months (waiting for integration), it has not recognized the merit of the Italian school for having placed correctly the problem still in the Sixties of the last century.
Besides, without having the experience and refusing the appropriate tools, it claims to teach the techniques of immediate loading even to those who have successfully traveled this path several years earlier.
It is producing surprising guidelines which, if they can perhaps (because they have peri-implantitis and mucositis) be suitable for the use of implants with considerable volumes, super-technological in their constituent parts and in their macro and microscopic structure, are limiting for the technique implant of the Italian school that uses slimmer implants. These guidelines, therefore, cannot be adopted in all types of systems.
The implants of the Italian school generally have a monobloc structure. In the last ECM course by Dental Cadmos which we attended last December, we read with surprise that immediate post-extraction implants undergo dehiscences with a very high frequency (up to 64%): Prevalence in the literature of TMDs, especially soft tissue dehiscences when immediate post-extraction implants are performed. Authors of reference: Martina Stefanini, researcher DIBINEM Univ. Di Bologna, Giovanni Zucchelli full professor DIBINEM univ. Di Bologna in THE MANAGEMENT OF PERI-IMPLANT SOFT TISSUE COURSE ECM PROVIDER: IMAGE OF 2020. We have different data. In the last 33 years of activity we remember less than ten cases with dehiscences in anterior peri-implant areas related to Tramonte implants. With about 5000 implants inserted. We will provide the reference data as soon as possible. Why?
|
Date Year 1991 |
|
Clinic: Cavriana of Dr. Bellini Maria Angela |
|
surname and name: Xxxxxxx Xxxxxx |
|
Age: 41 years |
|
N ° existing plants: 0 |
|
Date and number of interventions already made: 0 |
|
Type of plant: Tramonte plant |
|
N ° implants inserted: 1 |
|
Welding: No |
|
Dental area: 46 |
|
App. Intraoral Rx: Vix Win Cavriana |
|
CT scan: no |
|
Extractive situation: immediate post-extraction implant and immediately loaded |
|
Density according to Misch: D2 |
|
Antagonist of natural fixed elements, implants or mobile prostheses: natural elements |
|
Thick mucosa thickness medium thin: medium. |
|
Chewing height high medium low: medium |
|
Bruxism: No |
|
Photo |
|
Models: yes |
|
Consent / Information: yes |
|
Privacy |
|
Operator 1: Dr. Bazzoli F. |
|
Operator 2: Dr. Bellini MA |
|
Drill sequence: Lanceolata only |
|
Sequence of taps: tap diameter 5 mm |
|
Occlusal loading: Immediate, slightly unloaded. |
|
Intervention description |
|
Complications: absent - |
|
Video or written statement of satisfaction: yes |
The stem, the coils, how much bone to remove.
This has been the main road taken by a good part of the Italian school: to use screws with a similar design to that used in wood screws. With this technique, the tapper does not remove shavings, but carves the bone, incising it and during penetration it compresses it slightly, compacting the first outer layer of bone. It thus contributes to increasing primary mechanical stability; obviously the displacement of the trabeculae strictly adjacent to the tapper is allowed by the physiological presence of the spaces between them. The only drill used in 90% of cases, the lanceolate drill, like the tap, does not remove bone but compacts it on the external surface of the implant tunnel. Only some frustules remain adherent to the cutter when it is withdrawn.
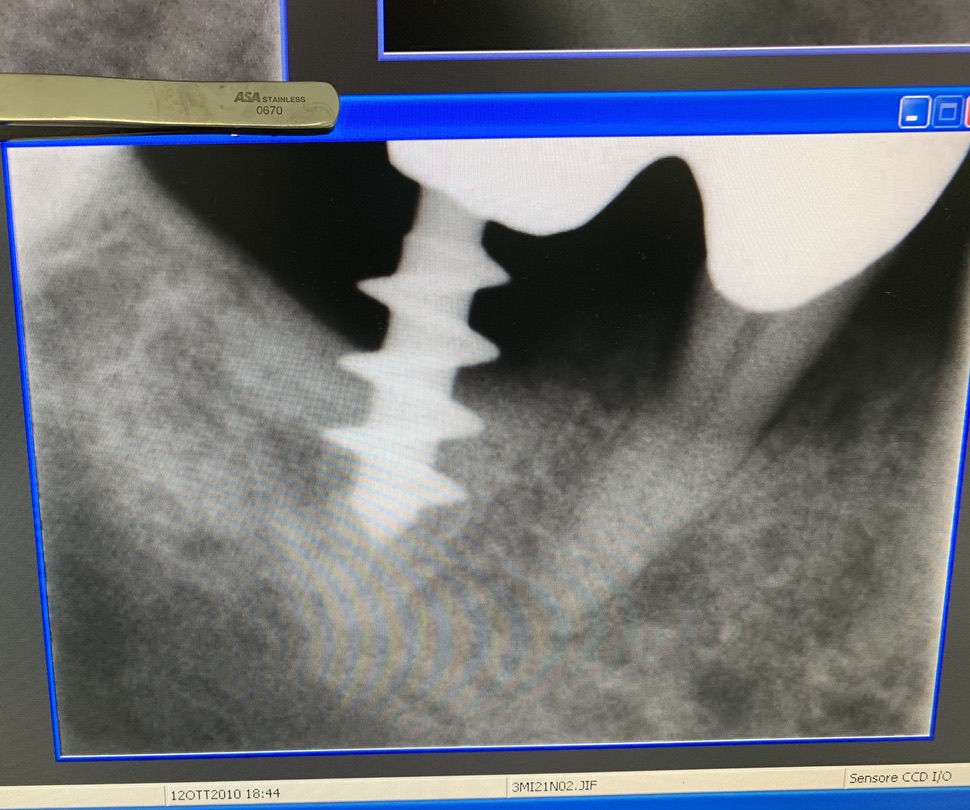
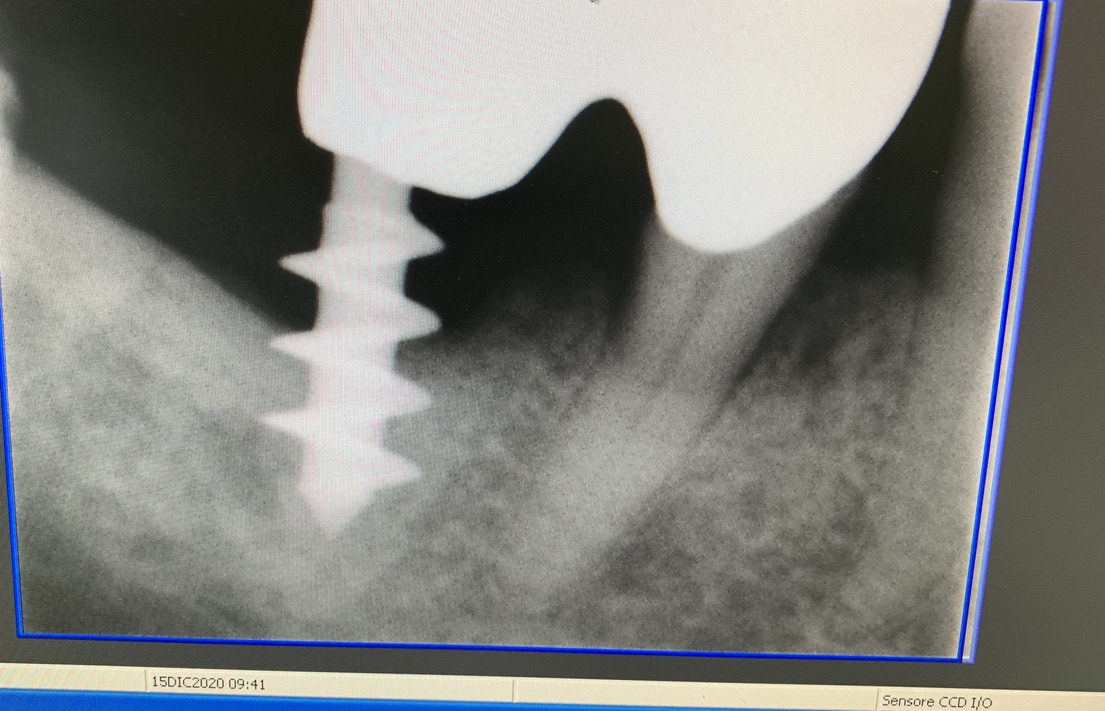
Original form of the Tramonte implant. 5 mm diameter with 3 threads. Stem diam. 2.1 mm. Neck diam. 2 mm x 5 mm in length. Grade 2 titanium. Grade 2 allowed the need to bend the implant neck to improve parallelism. It is an immediate post-extraction implant. Therefore, in the same session, extraction, boring, tapping and implant insertion. Immediately followed by monconization and the preparation of temporary crowns in light occlusion. The radiographs provided show the situation since 2010. The emergence of the thin neck favors the formation of a dense gingiva sleeve that protects against peri implantitis. The wide threads radiate the occlusal load away from the implant body, favoring the formation of a more homogeneous bone.
Bazzoli Francesco Bellini Maria Angela.




STUDI DENTISTICI BAZZOLI e BELLINI
Privacy Policy e Cookie Policy
Internet Partner Global Informatica
![]()