12 - IMPLANT RITUALITIES
PRELIMINARY
- Open the CT scan on the screen with the sections in which you work. Re-evaluation of height, thickness, inclination, density, structural details, thickness and course of the cortices, course of the mandibular canal in the mandible, its dimensions and any splitting, course of the maxillary sinus floor, of the nasal floor, structure of the tuber where necessary for the maxillary.
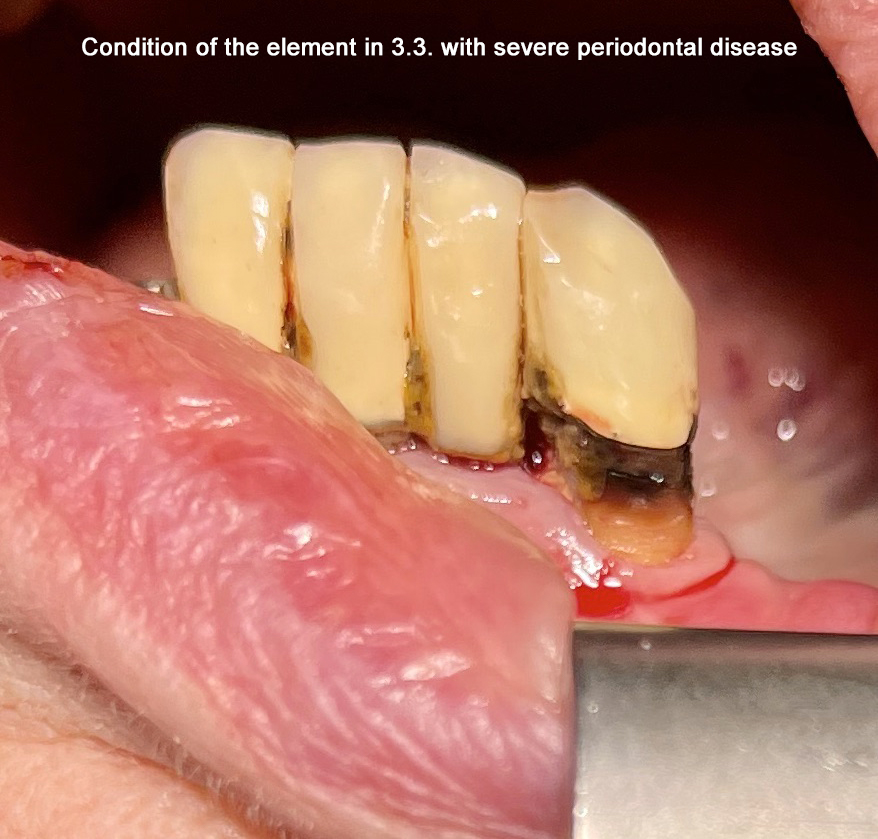
- Open the intraoral X-ray to see the initial situation, in particular undercuts of the roots to be extracted, apical radiolucencies, presence of severe periodontal diseases, bearing in mind the frequency of repetition of abscess episodes if present.
- Photos of the operating field and of the antagonist, mobile, fixed.
- Rinse with chlorhexidine.
- Did you take the antibiotic this morning?
- Patient well positioned in chair with extended head.
- Operator who occupies the most suitable ergonomic position to follow the orientation of the bone during work.
- Palpation that confirms the CT data regarding the shape and course of the bone, the presence of adherent gingiva, intermaxillary relationships and residual occlusal space to confirm the height of the abutment.
- Minimal anesthesia, aimed with peripress or with a straight syringe only in the operative area.
- Gentle extraction of the element or root avoiding trauma.
- Curettage of the alveolus bottom if necessary.
- Rx of the extracted area.
- First wash with Rifocin.
REAL IMPLANTOLOGY
- If it is not post-extraction and if there is an occlusal cortex or a narrow crest tungsten bur to create the entry site.
- Low speed spear cutter.
- Washing with refocin.
- When necessary Rx with the lanceolate cutter inserted and take the length measurement.
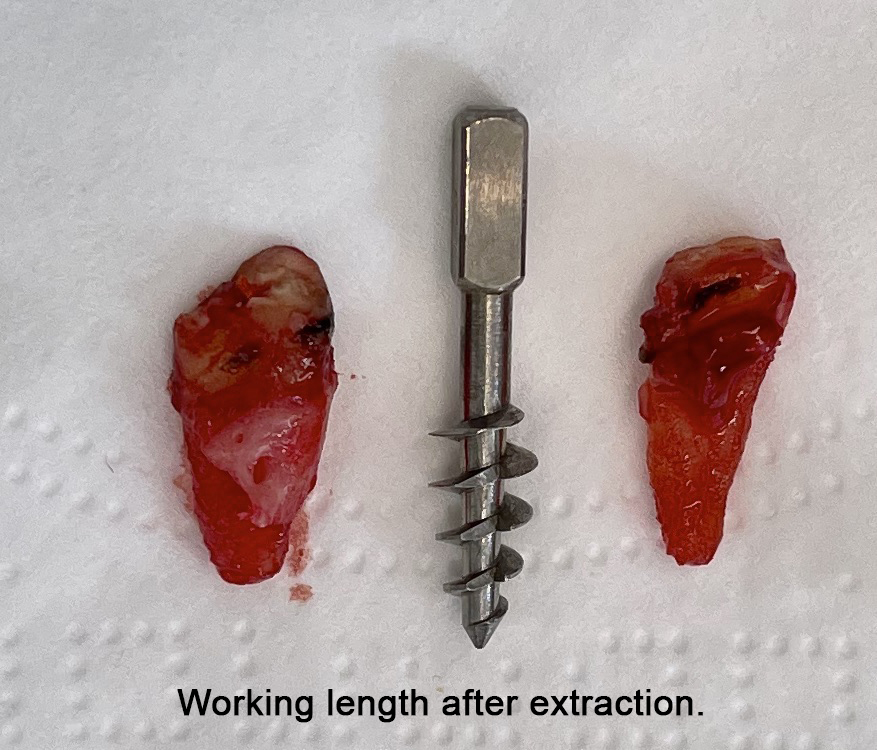
- Photo of the length of the drill with the root and an implant as a reference to establish the implant dimensions.
- If the bone density appeared consistent, tapping with a diam. 4.
- Washing with refocin. X-ray of the depth reached by the tap.
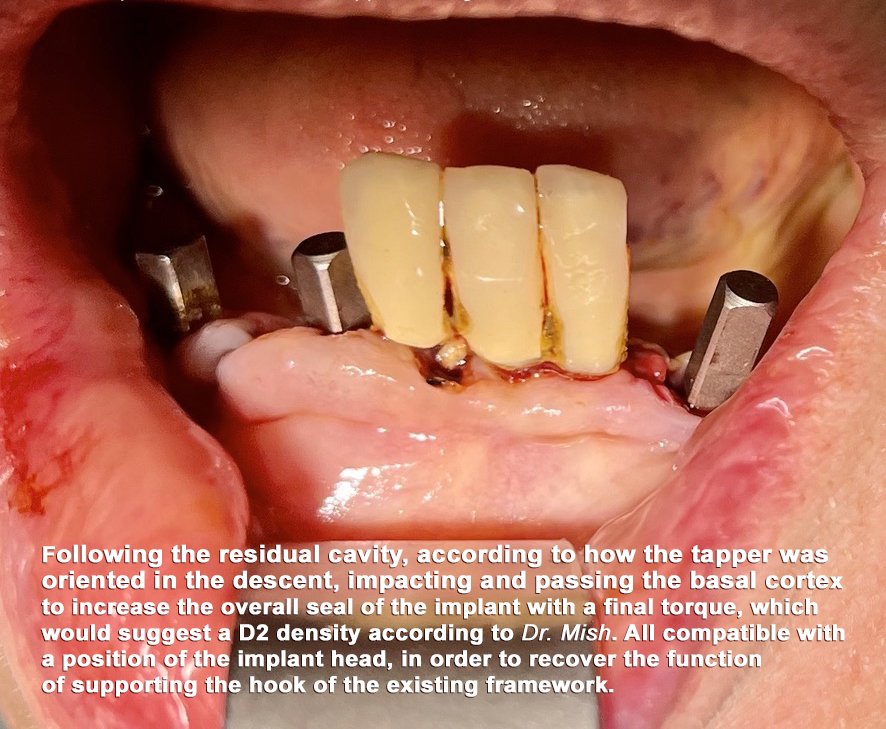
- Insertion of the 5 mm tap with cavitation risk assessment Tapping with a 5 mm diameter tap with evaluation of the insertion torque at various depth levels Washing with refocin.
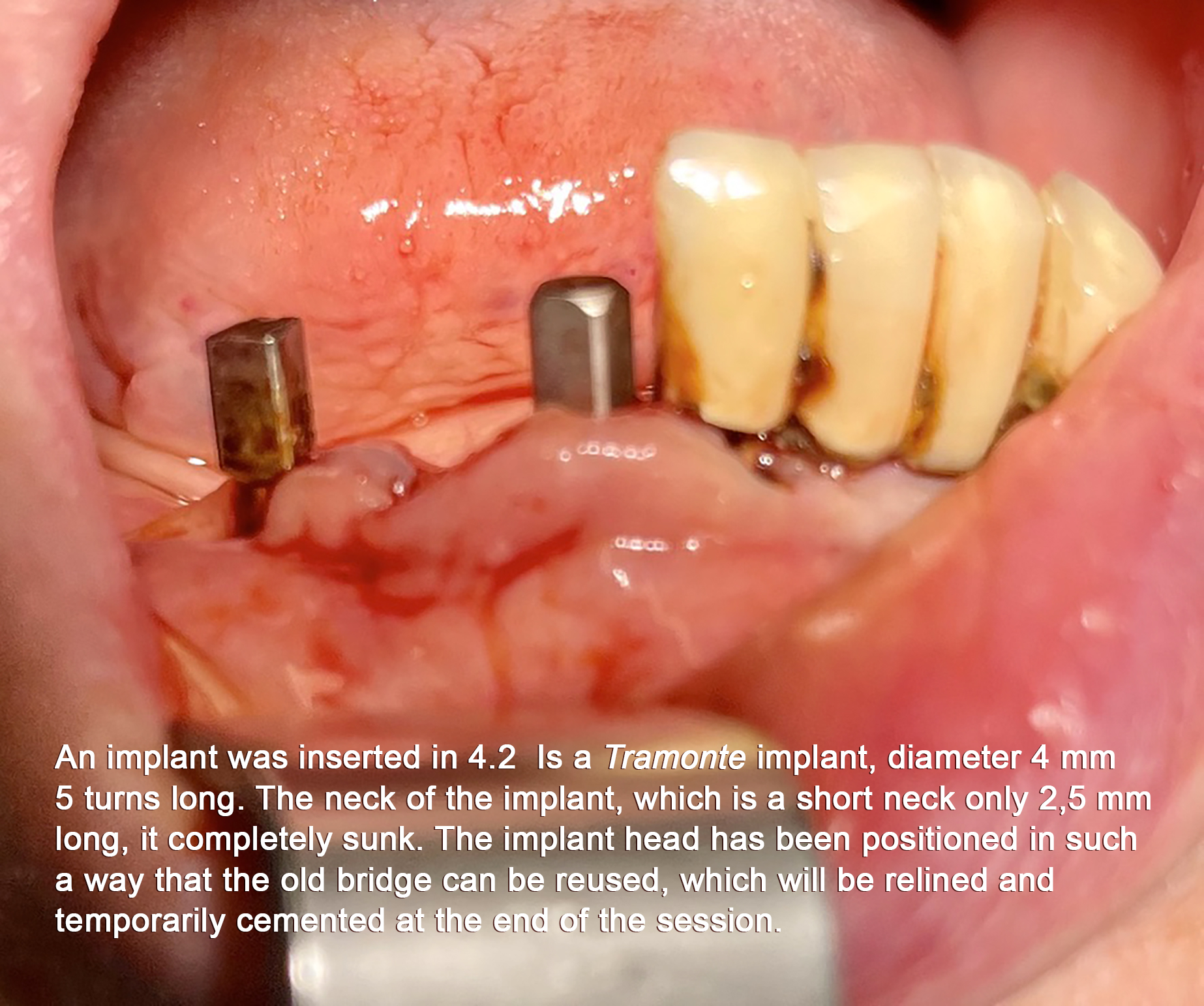
- Choice of implant: diameter and number of threads.
- Resterilization of the system in the quartz pellet sterilizer.
- Implant insertion with a manual screwdriver and / or ratchet. The insertion must be smooth, making sure that the threads deepen into the implant tunnel.
- Check that the implant neck is well sunk.
- Final Rx.
PROSTHETIC PART
- Mononize the implant by parallelizing it with other natural / implant elements present.
- Leave adequate spaces in occlusion.
- Prepare the provisional, finish it, in the gingival, in the vestibule / lingual, in occlusion plus shape of the cusps.
- The occlusion must be light, or slightly discharged, punctiform with a reduced occlusal plane. Plan of the junctions reduced in height.
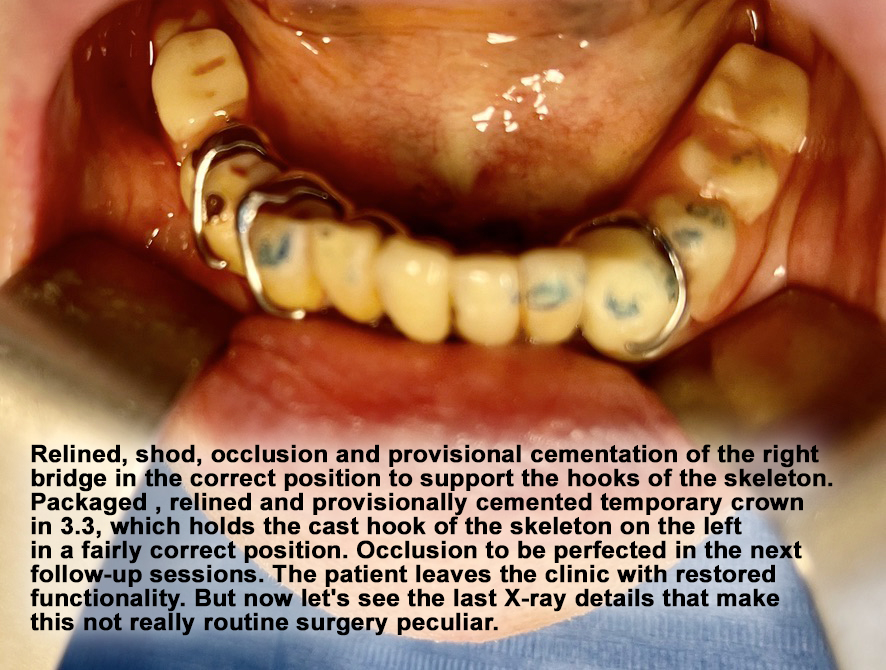
- If there is no primary retention, proceed with the relining by finishing it and / or provisionally cementing the framework.
- During the various phases, photographically document the salient moments.
- If the affected area was later than 34/44, check for signs of the return to normal sensitivity (see later). FINAL RECOMMENDATIONS of therapy: antibiotic, anti-inflammatory, ice. power supply. work behavior. Make a new check-up appointment. Record the intervention in the folder and report all the key data in the Plant Register.
Other Ritual Aspects of Contemporary Implantology...
STERILITY
What do you use to sterilize the irons? Class B autoclave, pellet sterilizer. Ultrasound, iron bath in germicidal solutions? All these things together?
Non-provocative question: If a lever or a mirror falls on the ground, what do you do? Do you return it to the supplier to have it replaced sterile? But if: If the system you plan to use falls on the ground, what are you doing? .......
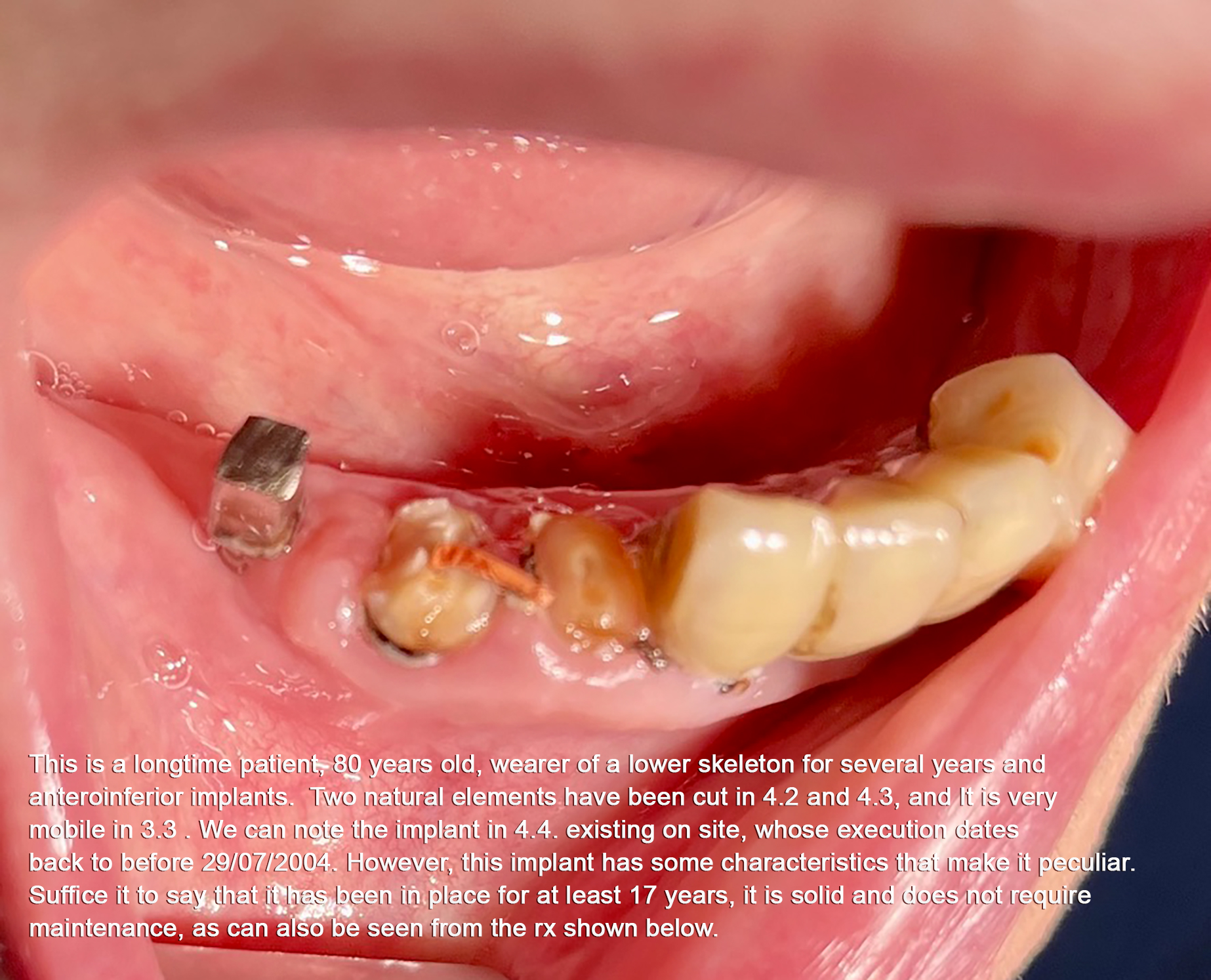
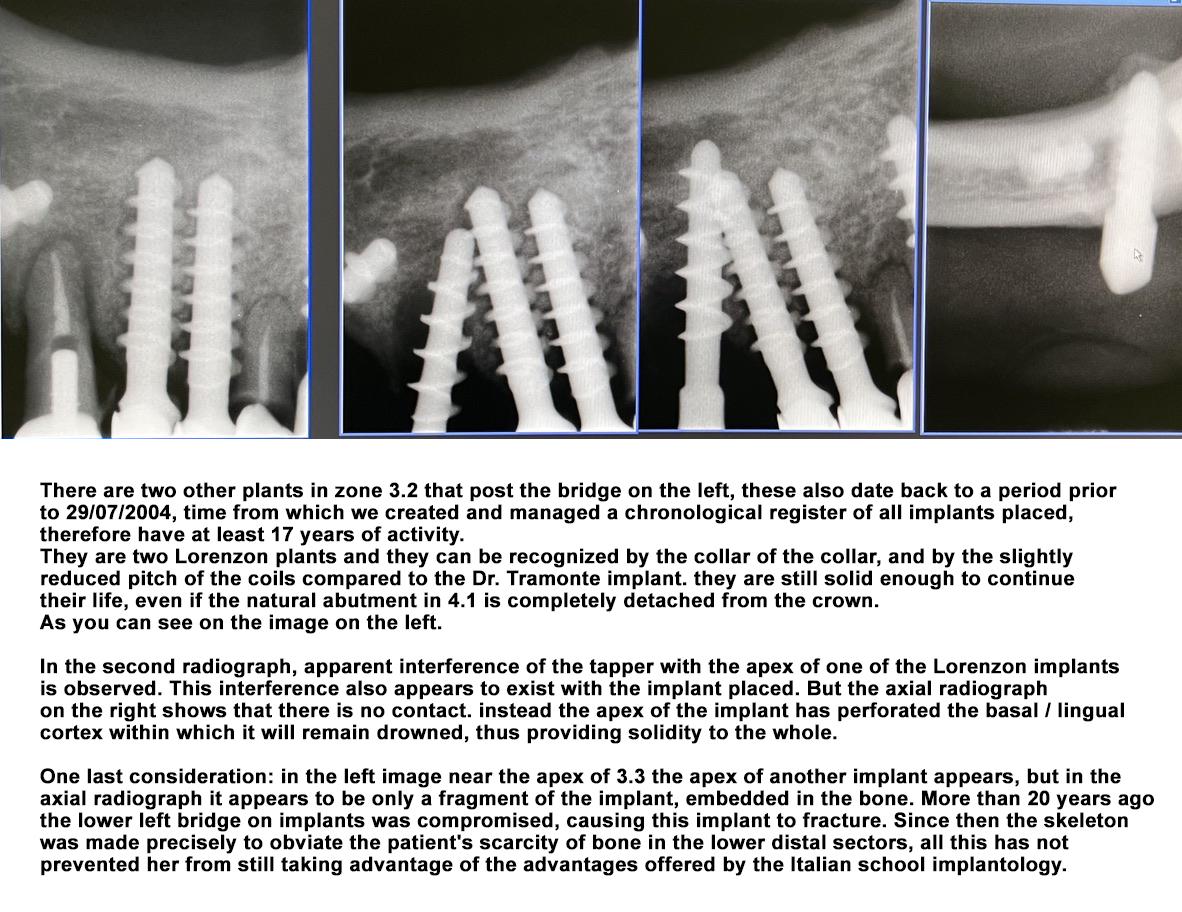
Other question: you bought 5 implants of various sizes and lengths. During the surgery you realize that you do not have the right implant: you need a shorter one because you are too close to the mandibular canal. What are you doing? Do you postpone the appointment and the intervention while you wait for the fastest courier to deliver you in record time? Are you happy with a less performing system if you have it? Or shorten your system !!! .... Knowing how to do it naturally. But .. is it possible to shorten or modify the system? And how long does an implant shortened in the correct way last?
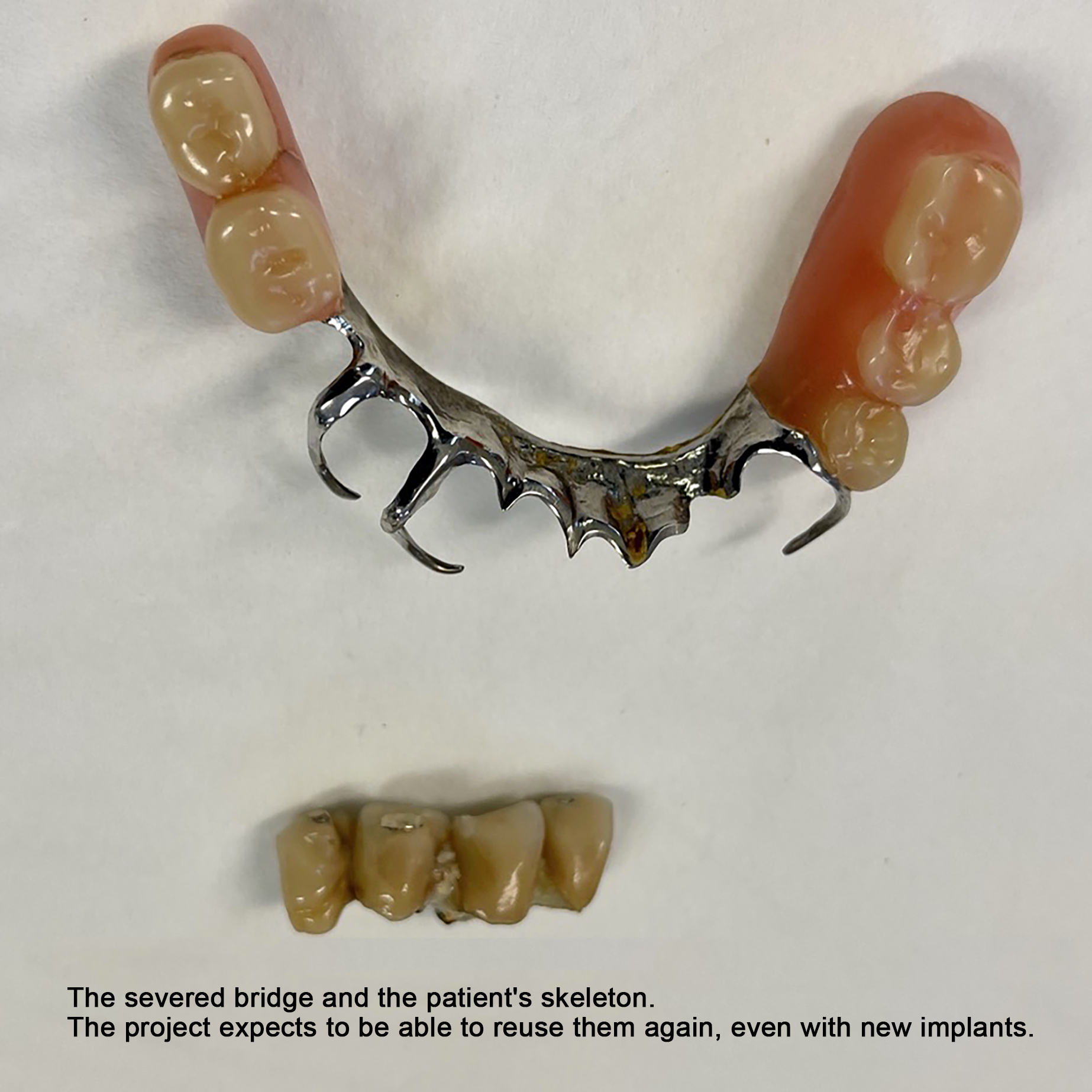
A partial answer can be found in the following clinical case, recently performed.



STUDI DENTISTICI BAZZOLI e BELLINI
Privacy Policy e Cookie Policy
Internet Partner Global Informatica
![]()