11 - CONDITIONS OF STERILITY
STERILE SURGERY, CLEAN CONTAMINATED SURGERY
The topic of the type of surgery to be used during implant surgery deserves a not without importance. As is known and as the Mish and Chiapasco themselves recall in their books, which are very complete, (see page 348 of Misch and page 107 of Chiapasco), there is an ongoing controversy regarding the sterile surgical technique with respect to to clean technique in the insertion of bone implants. '.... The clinical decision for a sterile rather than clean environment remains a decision of the individual operator since there is documentation for both approaches ......... Intraoral surgery is assimilated to a class II or clean contaminated surgery. However, it is prudent to reduce the risk of infection .... '.
The adoption of more invasive procedures therefore requires more virtuous, 'more sterile' behaviors which naturally involve more rigid protocols, complicated by greater preparation and education of all team members, and more time to be made available for the organization of the surgery. In this context, it is understood, after having made an effort to achieve conditions of sterility, however unattainable in the oral cavity, how serious it is to allow intra-implant spaces to be colonized indefinitely by saprophytic bacteria of the oral cavity. In the same way, extending the surgical field with unnecessary detachments, osteotomies or bone grafts of uncertain prognosis, lengthens the healing times, while increasing the infectious risk of the surgical site and consequently the rules of sterility to be adopted. Thanks to the mini-invasiveness of the Italian technique, we found it unnecessary and inappropriate to adopt sterile techniques in our interventions. Since 1986, after a possible rinsing with chlorhexidine, under antibiotic coverage, and after intraoperative washes with rifocin during the operation, we have never recorded complications related to sterility problems.
At the end of these brief considerations it might be appropriate to evaluate the following behaviors in implantology. I met 'surgeons' who, having dropped an implant on the floor, had it replaced by the supplier. We personally adopt the correct procedure of resterilizing the implants at 350 ° in the quartz ball sterilizer for 8 seconds, then cooling it in the air for 10 seconds and then in a Rifocin bath. Our clinics are equipped with the latest generation type B autoclaves. We currently use ultrasound and germicidal liquid baths for all our instruments.
|
Data 19/04/2021 |
Ambulatorio Acquafredda |
Cognome e nome: Xxxxxx Xxxxx |
Età 64 |
|
N.impianti esistenti: 2 |
Data e n.interventi già fatti: 2010 in 22. 2013 in 12 |
||
|
Tipo di impianto: Tramonte |
N.impianti inseriti: 2 |
Saldatura: no |
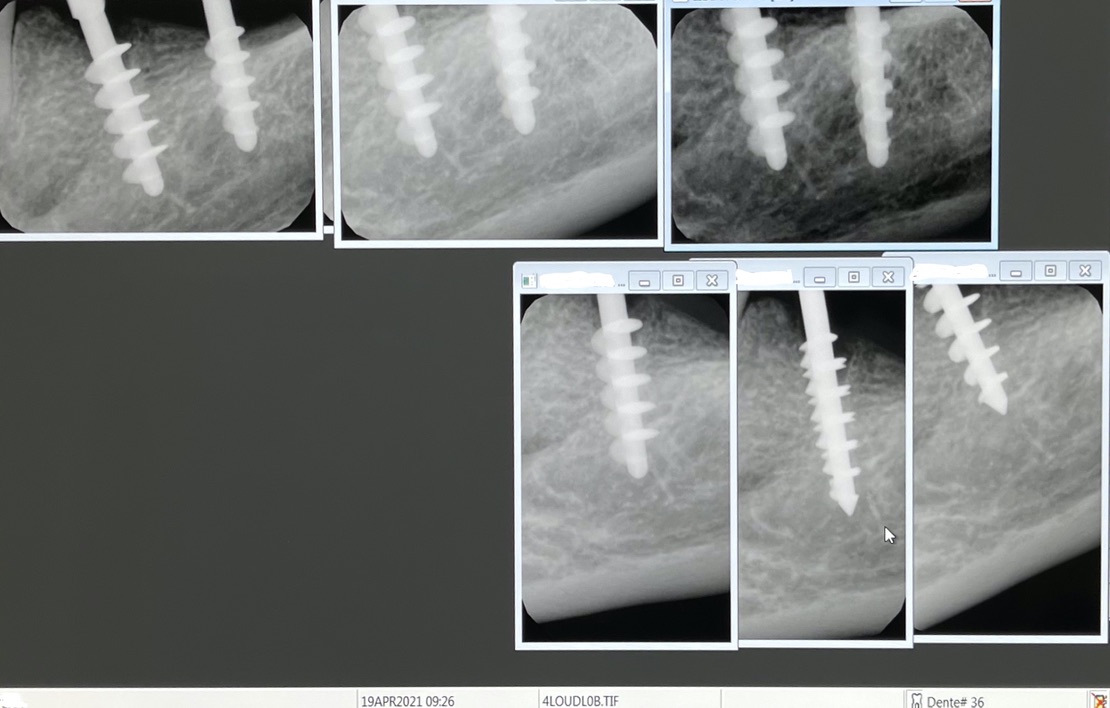
Zona dentale: 35 - 36 |
|
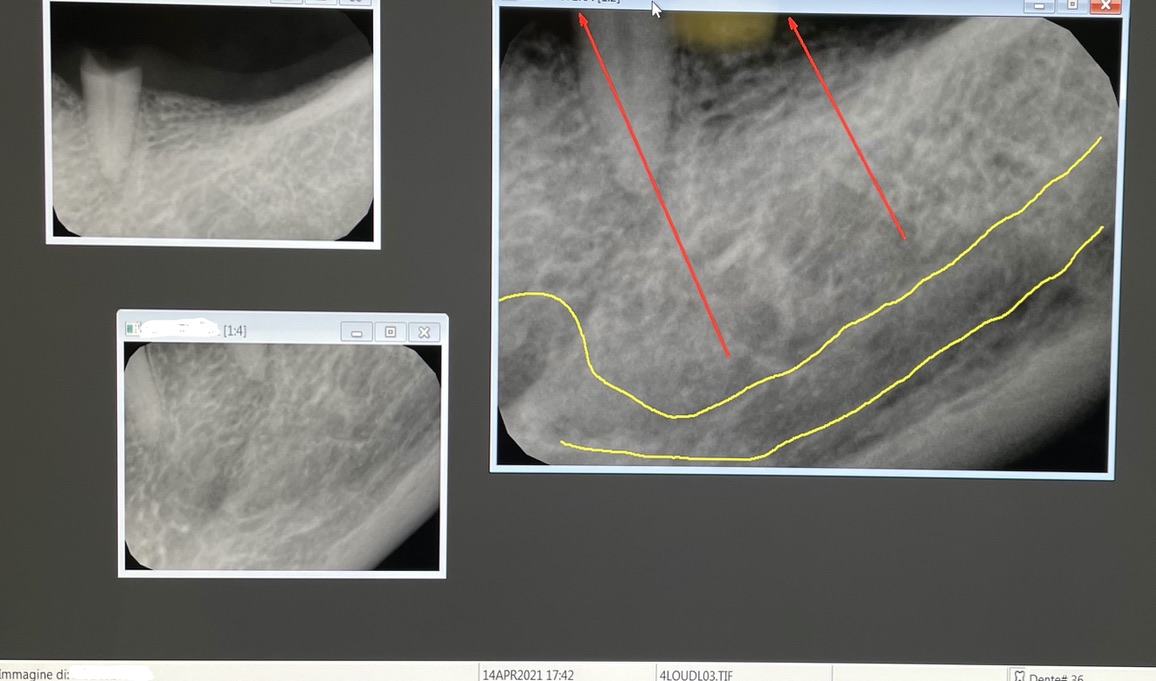
App.Rx endorale: Vix-win Acquafredda |
Tac: no |
Situaz.estrattiva: pexist in 35 nopex in 36 |
Densità secondo Misch: D2 |
|
Antagonista(fissi,mobili,naturali,implantari: naturale |
Spessore mucosa: normale |
Altezza masticazione: media |
Bruxismo: assente |
|
Foto : Iphone 12 |
Modelli: no |
Consenso/informativa: si |
Privacy: si |
|
Operatore 1: dr. Bazzoli F |
Operatore2: dr. Bellini MA |
Sequenza frese: solo lanceolata |
Sequenza maschiatori: diam. 5 in 35 e diam. 4 in 36 |
|
Carico occlusale: immediato leggero |
Complicanze: nessuna. Sensibilità restituita a fine intervento. |








STUDI DENTISTICI BAZZOLI e BELLINI
Privacy Policy e Cookie Policy
Internet Partner Global Informatica
![]()