10 - MECHANICAL ASPECTS: THIKNESSES AND FRACTURES, TORQUE AND CAVITATION
FRACTURES AND DEFORMATIONS
A problem arising from the use of cable implants, which is rarely talked about, concerns the torque to be exercised while screwing the implant; in fact, by recommending the use of torque wrenches and not to exceed 30 Newtons of torque, surgical protocols very often neglect to report the risk of triggering fractures and irreversible deformations in the implant itself. It has a very articulated internal morphology and also has very thin thicknesses and anfractuosity sensitive to stress from screwing with deformations which can occur at the time of inserting the healing screw, at the moment of loading the implant, or at a distance of time.Unfortunately, the intra-implant cavities constitute a reservoir of bacteria placed under the mucosa and have their responsibility in the development of peri-implantitis, with consequent inflammation of the mucosa and bone resorption over time.
CAVITATION
You made the hole with the spear drill, correct buccolingual inclination. Centered disto mesial position. You start tapping, go down a little, continue to turn the manual screwdriver, or the ratchet; how beautiful! Everything good. I am an implantologist ... Suddenly you realize that the tap has not come down. Or maybe you realize after two full turns that it hadn't advanced into the bone canal. Disaster!! You caved in !. If you remove the tapper, and worse if it was the implant, you see a red pulp between the coils, fragments of bone. Good boy!! Precisely that was the bone to which the implant had to be anchored through the coils and through this download the forces ......... Now in the affected section you no longer have a 2 mm hole to tap and create the sirloin in it, but a 4 mm tunnel if you used a 4 mm tap. Or you have a nice 5 mm hole if you used a tap or a 5 mm diameter implant. Goodbye immediate stability, goodbye immediate loading !! ..... The tightness of your screw has become zero as if it were an old cork in a bottleneck.If the bone in height was little, only for two turns or three you you are gambled the chance to place the implant. You have forgotten an important thing: the screw you use is a machine that must advance while it turns, but if after a full turn it has not dropped by 2.2 mm, instead of penetrating by anchoring, it has chopped the surrounding bone !!!! Exactly like grandfather's meat grinder to make salami. Sic ..
If you are using diameters greater than 6, 8 or 10 mm the damage is in proportion. Therefore, when using the tap, push hard but rotate slowly. Push hard and in line with the patient's head, who you will have advised to stay still, immobile and in the meantime make sure that you are actually descending, along the chosen direction. For this purpose, make sure that nothing disturbs your operation. Warn those around you. No aspirator that suddenly moves, no lip puller that moves, no variation of light because some head is interposed to look better. The field must be dry, without buds. Keep in mind that this mess can always happen to you with any implant even if you have already made ten thousand of them. Watch the x-rays carefully for thickening of the medullary bone that you may not have noticed before. If there is an increase in density you have to increase the penetration force, so push but turn slowly. Excess thrust does no harm, it helps the descent. The absence of the thrust, on the contrary, forces the coil to move forward making all the effort to the section of bone in which it is engaging which therefore can crumble as it turns.
Now you can tell the patient: 'He sees the bone doesn't hold. The implant cannot be done ". Or: "you see we can't do immediate loading, we have to wait three months and use an osseointegrated implant which is safer ......" or other pearls of the same type. If you don't immediately notice the trouble you have made, after a few months you can always say: “You see, three months have passed and he has not yet integrated. There was rejection ". Let's get back to us. When, after successful tapping, you begin to screw the implant, you must feel with your fingers that the implant is descending and runs through the newly created canal. Now you have to be gentle, minimal push and watch the descent. Maintain the same axis of penetration as there was before. Even the most cooperative patient, believing he is helping you, or if he is in pain, twists his head and changes your position space of the implant path and makes you jam the descent. Eye to ergonomics. But we'll talk about it again ... now you will say: but the 30 Newton of torque?
|
Data 02/03/2021 Ambulatorio Guidizzolo |
|
|
cognome e nome Xxxxxxx Xxxxx |
Età 75 anni |
|
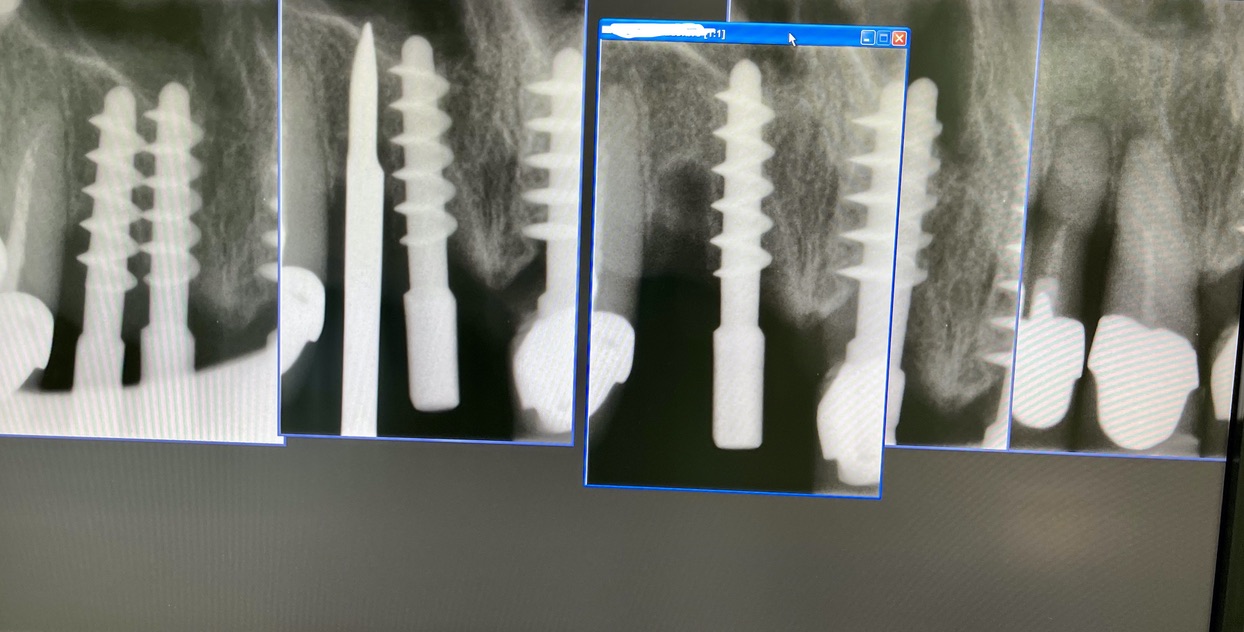
N° impianti esistenti 10 |
Data e n°interventi fatti: 2014:35 44 45 46. 2016: 16. 2017:22 23 24 25. 2019: 21 |
|
Tipo di impianto Tramonte |
N° impianti inseriti : 2 |
|
Saldatura no |
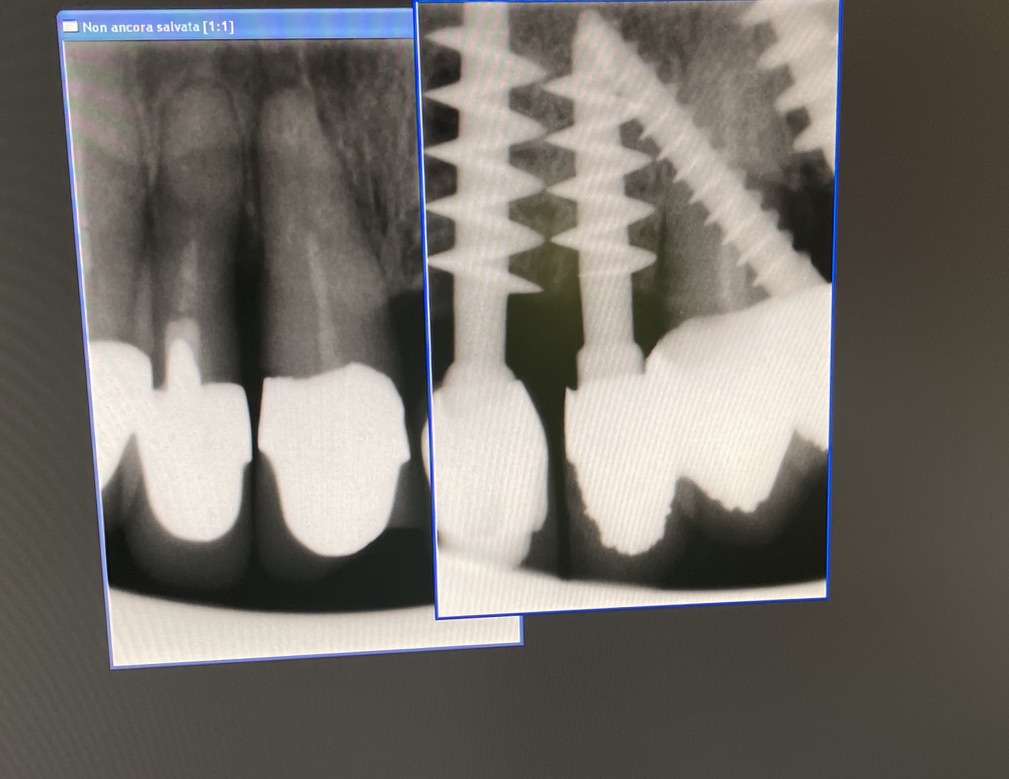
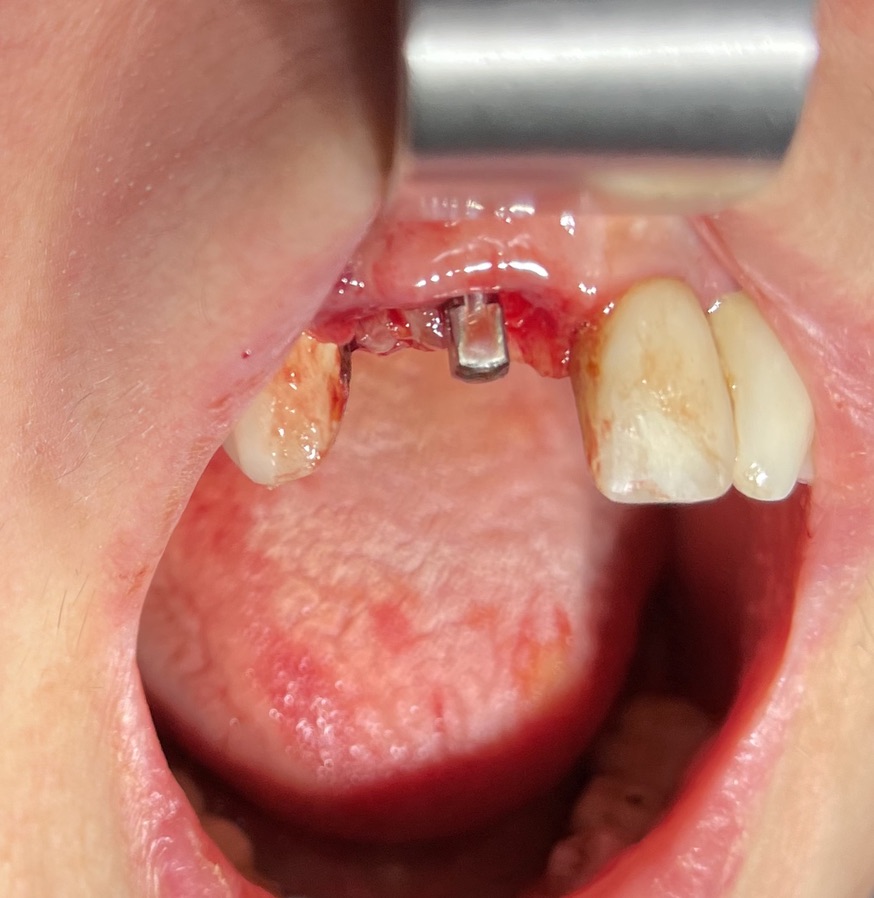
Zona dentale: 11 12 |
|
App. Rx endorale : vix win Guidizzxolo |
TAC: presente |
|
Situazione estrattiva: postestrattivi immediati |
Densità secondo Misch: D2, D3 |
|
Antagonista elementi fissi naturali,implantari o protesi mobile: naturale |
Spessore della mucosa spessa media sottil: media |
|
Altezza di masticazione alta media bassa: bassa morso profondo |
Bruxismo: assente |
|
Foto : iPhone 12 |
Modelli: presenti |
|
Consenso/Informativa si |
Privacy: si |
|
Operatore 1: Dr. Bellini |
Operatore 2: dr. Bazzoli |
|
Sequenza frese: solo lanceolata |
Sequenza maschiatori: diametro 4 mm |
|
Carico occlusale : immediato leggero |
Dichiarazione di soddisfazione video o scritto: scritto presente |
|
Descrizione intervento |
Complicanze: assenti |






STUDI DENTISTICI BAZZOLI e BELLINI
Privacy Policy e Cookie Policy
Internet Partner Global Informatica
![]()